From: MedScape Medical news (login required).
More than 123.8 million people in the United States will make an ED visit, and 13% will end up being admitted to the hospital, according to the US Centers for Disease Control and Prevention.
Researchers analyzed more than 7 million Medicare patient records from 2008 to 2010 for 12 diagnoses: bowel obstruction, chronic obstructive pulmonary disease, diabetic acidosis and coma, gastrointestinal bleed, myocardial infarction, heart failure, pancreatitis, pneumonia, pulmonary embolism, respiratory failure, sepsis, and stroke.
Medicare patients admitted to the nation's best-performing hospitals for emergency medicine have a 40% lower death rate compared with all other hospitals, according to a new survey by HealthGrades, a Denver, Colorado–based provider of information about physicians and hospitals.
"If all hospitals performed at the level of the Emergency Medicine Excellence hospitals from 2008 through 2010, an additional 170,856 people could have potentially survived their emergency hospitalization," the HealthGrades release notes.
In the Bay Area, 6 Hospitals were in the top 5%.
For other States, please follow this link.

Welcome to my blog ! My goal is to educate the public on chiropractic and medical issues, exciting and new therapies, medical research and health & wellness tips.
Wednesday, April 18, 2012
Tuesday, April 17, 2012
Who will have Health Insurance in the future ?
From: Annals of Family Medicine. 2012;10(2):156-162.
It was previously estimated that the cost of a family health insurance premium would equal the median household income by the year 2025 by DeVoe and colleagues.
In an updated model, it is estimated that this threshold (i.e. the cost of a family health insurance premium would equal the median household income) will be crossed in 2033, with a "best case scenerio" that the PPACA (Patient Protection Affordable Care Act) may extend this date only to 2037.
When did Insurance Premiums rise to these historic levels ?
In the "managed care" era of the 1990's, health care inflation slowed. However, there was a public backlash and many employers had abandoned that model. In 1999, there was a steep increase in health insurance premium inflation, coupled with declining inflation in household incomes.
The passage of the Patient Protection and Affordable Care Act:
Interestingly enough, when there was debate in congress regarding health care reform in 2009/2010, health insurance premium inflation had slowed to levels not seen since the 1990's. Despite this slowing, the annual inflation rate of health insurance premiums still outpaced US household earnings, which stagnated from 2008 to 2011 and included an absolute reduction in average household income from $50,300 in 2008 to $49,800 in 2009. Therefore, as median household incomes decreased, healthcare premium inflation had increased.
The passing of the PPACA in 2010 saw the number of persons without health insurance in the United States rise to a historic high of 50.7 million people after 5 million Americans lost employment-based health insurance in the 2007–2009 recession. The irony of this was that the PPACA was supposed to reduce the number of uninsured. This can be explained by the language of the PPACA which is supposed to take place over several years however.
Model of median household income and health insurance premium increases:
In this model, from 2000 - 2009, health care premiums and median household incomes were compared. The average annual increase in insurance premiums was 8.0%; household incomes rose an average of 2.1%.
If health insurance premiums and national wages continue to grow at recent rates and the US health system makes no major structural changes, the average cost of a family health insurance premium will equal 50% of the household income by the year 2021, and surpass the average household income by the year 2033. If out-of-pocket costs are added to the premium costs, the 50% threshold is crossed by 2018 and exceeds household income by 2030.
Factoring in employers contribution:
Since most workers do not pay for the entire cost of healthcare, the model was updated to include employers contribution to family healthcare. The average amount an employee pays for a family health insurance premium plus out-of-pocket family health care expenses was factored in. Without major structural changes in the US health care system, the employee contribution to a family premium plus out-of-pocket costs will comprise one-half the household income by 2031 and total income by 2042.
What is the effect with the passage of the PPACA:
There is no consensus among experts regarding the effect of the PPACA with regards to increasing or decreasing the costs on private health insurance. Assuming the PPACA actually slows cost growth, this threshold of insurance premiums exceeding household income is delayed only by 4 years.
What are Insurance Companies and employers doing to curb costs:
Employee contributions to insurance premiums and out-of-pocket expenses have grown faster than overall premium costs, suggesting that insurers have slowed the rate of growth in premiums by shifting more costs onto patients. Even though patients no longer face double-digit increases in insurance premiums each year, they now pay higher deductibles and co-payments and receive fewer covered services.
In a 2010 Kaiser Family Foundation and Health Research and Educational Trust employer survey:
30% of employers reported having reduced the scope of health benefits or increased cost sharing.
23% increased the share of the premium a worker has to pay.
Among large firms (200 or more workers):'
38% reported reducing the scope of benefits or increasing cost sharing, up from 22% in 2009.
36% reported increasing their workers' premium share, up from 22% in 2009.
Healthcare as a part of our GDP:
Health care continues to comprise a growing portion of the total US economy. It has risen from 13.7% of gross domestic product (GDP) in 2000 to 17.3% of GDP in 2010. From 1960 to 1999, the growth of national health care expenditures exceeded the GDP by 2.4% per year. This same 2.4% differential occurred from 2000 to 2009. If health care costs continue to rise at current unsustainable rates, it is doubtful that affordable insurance coverage will be available for low-to middle-income Americans in the near future. Further, our model did not include the taxes paid by American workers each year to finance Medicare and Medicaid—nearly $900 billion in 2009—which may increase with the PPACA.
How does our Healthcare policies affect other aspects of the economy:
It has been observed that expensive US health care increases production costs and makes American manufactured goods less competitive, which results in lower wages and fewer jobs in the manufacturing industry. For example in 2006, General Motors' spent $1,500 more than Toyota in health care costs per car.
It was previously estimated that the cost of a family health insurance premium would equal the median household income by the year 2025 by DeVoe and colleagues.
In an updated model, it is estimated that this threshold (i.e. the cost of a family health insurance premium would equal the median household income) will be crossed in 2033, with a "best case scenerio" that the PPACA (Patient Protection Affordable Care Act) may extend this date only to 2037.
When did Insurance Premiums rise to these historic levels ?
In the "managed care" era of the 1990's, health care inflation slowed. However, there was a public backlash and many employers had abandoned that model. In 1999, there was a steep increase in health insurance premium inflation, coupled with declining inflation in household incomes.
The passage of the Patient Protection and Affordable Care Act:
Interestingly enough, when there was debate in congress regarding health care reform in 2009/2010, health insurance premium inflation had slowed to levels not seen since the 1990's. Despite this slowing, the annual inflation rate of health insurance premiums still outpaced US household earnings, which stagnated from 2008 to 2011 and included an absolute reduction in average household income from $50,300 in 2008 to $49,800 in 2009. Therefore, as median household incomes decreased, healthcare premium inflation had increased.
The passing of the PPACA in 2010 saw the number of persons without health insurance in the United States rise to a historic high of 50.7 million people after 5 million Americans lost employment-based health insurance in the 2007–2009 recession. The irony of this was that the PPACA was supposed to reduce the number of uninsured. This can be explained by the language of the PPACA which is supposed to take place over several years however.
Model of median household income and health insurance premium increases:
In this model, from 2000 - 2009, health care premiums and median household incomes were compared. The average annual increase in insurance premiums was 8.0%; household incomes rose an average of 2.1%.
If health insurance premiums and national wages continue to grow at recent rates and the US health system makes no major structural changes, the average cost of a family health insurance premium will equal 50% of the household income by the year 2021, and surpass the average household income by the year 2033. If out-of-pocket costs are added to the premium costs, the 50% threshold is crossed by 2018 and exceeds household income by 2030.
Factoring in employers contribution:
Since most workers do not pay for the entire cost of healthcare, the model was updated to include employers contribution to family healthcare. The average amount an employee pays for a family health insurance premium plus out-of-pocket family health care expenses was factored in. Without major structural changes in the US health care system, the employee contribution to a family premium plus out-of-pocket costs will comprise one-half the household income by 2031 and total income by 2042.
What is the effect with the passage of the PPACA:
There is no consensus among experts regarding the effect of the PPACA with regards to increasing or decreasing the costs on private health insurance. Assuming the PPACA actually slows cost growth, this threshold of insurance premiums exceeding household income is delayed only by 4 years.
What are Insurance Companies and employers doing to curb costs:
Employee contributions to insurance premiums and out-of-pocket expenses have grown faster than overall premium costs, suggesting that insurers have slowed the rate of growth in premiums by shifting more costs onto patients. Even though patients no longer face double-digit increases in insurance premiums each year, they now pay higher deductibles and co-payments and receive fewer covered services.
In a 2010 Kaiser Family Foundation and Health Research and Educational Trust employer survey:
30% of employers reported having reduced the scope of health benefits or increased cost sharing.
23% increased the share of the premium a worker has to pay.
Among large firms (200 or more workers):'
38% reported reducing the scope of benefits or increasing cost sharing, up from 22% in 2009.
36% reported increasing their workers' premium share, up from 22% in 2009.
Healthcare as a part of our GDP:
Health care continues to comprise a growing portion of the total US economy. It has risen from 13.7% of gross domestic product (GDP) in 2000 to 17.3% of GDP in 2010. From 1960 to 1999, the growth of national health care expenditures exceeded the GDP by 2.4% per year. This same 2.4% differential occurred from 2000 to 2009. If health care costs continue to rise at current unsustainable rates, it is doubtful that affordable insurance coverage will be available for low-to middle-income Americans in the near future. Further, our model did not include the taxes paid by American workers each year to finance Medicare and Medicaid—nearly $900 billion in 2009—which may increase with the PPACA.
How does our Healthcare policies affect other aspects of the economy:
It has been observed that expensive US health care increases production costs and makes American manufactured goods less competitive, which results in lower wages and fewer jobs in the manufacturing industry. For example in 2006, General Motors' spent $1,500 more than Toyota in health care costs per car.
Doctors poll results on Affordable Care Act (ACA) aka "Obamacare"
From: WebMD, MedScape, business of medicine. Log in required.
The ACA is a hotly debated topic. Specifically, the individual mandate requiring individuals to purchase health care coverage. In fact, this will be debated in the Supreme Court this June.
Here are some of the highlights of the poll results from US Physicians:
The ACA is a hotly debated topic. Specifically, the individual mandate requiring individuals to purchase health care coverage. In fact, this will be debated in the Supreme Court this June.
Here are some of the highlights of the poll results from US Physicians:
Do you think it is or is not constitutional for the US government to require individuals to purchase healthcare insurance or else pay a penalty?
44% - Yes, it is constitutional
56% - No, it is not constitutional
Do you think all individuals should or should not be required to purchase healthcare insurance?
33% - It should be required; the ability to fund healthcare reform depends on instituting the individual mandate
14% - It should be required; it is wrong for uninsured persons to seek healthcare at emergency departments and then not pay
34% - It should not be required; the government should not force people to buy a product or service
18% - It should not be required; if healthcare reform cannot succeed without this mandate, then it is not a well-designed plan
Should the Supreme Court strike down the individual mandate but keep all other elements of the Affordable Care Act?
11% - Yes; the other policies of healthcare reform are useful, even if the individual mandate is eliminated
12% - Yes; even though the Affordable Care Act lacks a severability clause, the court can still selectively void inclusions of the mandate
51% - No; the overall economic structure of healthcare reform and the Affordable Care Act depends on the inclusion of the mandate
26% - No, because the Affordable Care Act lacks a severability clause that would preserve the rest of the law
Do you predict that the individual mandate will be upheld?
46% - Yes, it will be upheld
54% - No, it will not
Do you support or oppose the Affordable Care Act?
39% - Strongly support
8% - Somewhat support
4% - Neutral
43% - Strongly oppose
0% - Uncertain
Friday, December 16, 2011
Manipulation or Microdiskectomy for Sciatica ?
From: J Manipulative Physiol Ther. 2010 Oct;33(8):576-84.
Spinal manipulation (sometimes referred to as a 'spinal adjustment') is the Chiropractors primary therapy. Microdiscectomy is a surgical procedure which removes a portion of the facet joint (part of the spine) as well as a portion of the herniated disc which is "pinching" the nerve root.

This study concluded: "Sixty percent of patients with sciatica who had failed other medical management benefited from spinal manipulation to the same degree as if they underwent surgical intervention. Of 40% left unsatisfied, subsequent surgical intervention confers excellent outcome. Patients with symptomatic LDH failing medical management should consider spinal manipulation followed by surgery if warranted."
Conclusions: Have sciatica ? Considering the surgical options ? Why not try Chiropractic Spinal Manipulation which, according to this study, has a 60% chance of giving you the same outcome as if you were to have surgery. If all else fails, the surgical option is always available right ? Well, why not try non-surgical VAX-D Spinal Decompression Therapy.
Dr. Hindocha performs Chiropractic therapy and non-surgical Spinal Decompression therapy in San Mateo, California. Have you been diagnosed with Sciatica, a Herniated, Bulging or "Slipped" disc ? Call Peninsula Spine & Sports Rehabilitation at (650) 347-2225 to find out if you can benefit with Chiropractic care or VAX-D Spinal Decompression therapy.
Spinal manipulation (sometimes referred to as a 'spinal adjustment') is the Chiropractors primary therapy. Microdiscectomy is a surgical procedure which removes a portion of the facet joint (part of the spine) as well as a portion of the herniated disc which is "pinching" the nerve root.

This study concluded: "Sixty percent of patients with sciatica who had failed other medical management benefited from spinal manipulation to the same degree as if they underwent surgical intervention. Of 40% left unsatisfied, subsequent surgical intervention confers excellent outcome. Patients with symptomatic LDH failing medical management should consider spinal manipulation followed by surgery if warranted."
Conclusions: Have sciatica ? Considering the surgical options ? Why not try Chiropractic Spinal Manipulation which, according to this study, has a 60% chance of giving you the same outcome as if you were to have surgery. If all else fails, the surgical option is always available right ? Well, why not try non-surgical VAX-D Spinal Decompression Therapy.
Dr. Hindocha performs Chiropractic therapy and non-surgical Spinal Decompression therapy in San Mateo, California. Have you been diagnosed with Sciatica, a Herniated, Bulging or "Slipped" disc ? Call Peninsula Spine & Sports Rehabilitation at (650) 347-2225 to find out if you can benefit with Chiropractic care or VAX-D Spinal Decompression therapy.
Do Chiropractic Physician services for the treatment of Low Back and Neck Pain improve the value of health benefit plans ?

Traditionally, Doctors and Insurance plans have often disagreed on how to manage a patients health. For a Doctor, we recommend treatments and diagnostic testing (X-ray, MRI, CT, nerve testing) which we feel will give us the most accurate diagnosis and therefore formulate a treatment plan tailored to our patients needs. Insurance plans see their clients as liabilities and have therefore have hired third party individuals specifically to deny care and therefore cut costs of medically necessary treatment and diagnostics.
The Foundation for Chiropractic progress funded the following study to determine the COST SAVINGS to health benefit plans utilizing Chiropractic care for neck and low back complaints compared to Physician visits:
In a 2009 study titled "Do Chiropractic Physician Services for Treatment of Low Back and Neck Pain Improve the Value of Health Benefit Plans ? An Evidence-Based Assessment of Incremental Impact on Population Health and Total Health Care Spending" by Niteesh Choudhry, MD, PhD from Harvard Medical School and Arnold Milstein, MD, MPH from Mercer Health and Benefits, San Francisco concluded:
"When considering the effectiveness and cost together, chiropractic physician care for low back and neck pain is highly cost effective, [and] represents good value in comparison to medical physician care and to widely accepted cost-effectiveness thresholds. Because we were unable to incorporate savings in drug spending commonly associated with US chiropractic care, our estimate of its comparitive cost effectiveness is likely understated."
What was compared was the costs associated with Chiropractic physician care for episodes of neck and low back pain vs. costs associated with traditional Medical care (Medical doctor visits, Hospital visits, outpatient Physical Therapy and interventions). Note: the costs associated with medications WERE NOT factored into the calculations therefore the estimate of its comparitive cost effectiveness is likely understated.
Dr. Rommel Hindocha is a practicing Chiropractor in San Mateo. We offer quality Chiropractic care for neck and low back conditions. We are participating providers on most medical insurance plans including PPO, HMO, Kaiser, Workers Compensation and accepting automobile insurance plans (Medical Payments). If you, or someone you know, has a neck or low back complaint, call Dr. Hindocha at Peninsula Spine and Sports Rehabilitation in San Mateo at (650) 347-2225.
Tuesday, November 29, 2011
Whiplash - Cervical Zygapophysial Joint Pain After Whiplash
From: On Cervical Zygapophysial Joint Pain After Whiplash. Bogduk, Nikolai MD, PhD. Spine: 1 December 2011 - Volume 36 - Issue - p S194–S199.
What is Whiplash ?
Whiplash is an injury to the neck and upper back that can occur following an auto accident. Whiplash can also occur in other circumstances where the neck is forced backwards and then forwards such as a fall or during a sporting event. In automobile accidents, whiplash occurs as a result of sudden "acceleration - deceleration" forced to the spine and soft tissue structures (tendons, ligaments and muscles):
 Whiplash Associated Disorder (WAD), describes a more serious and chronic condition which can include symptoms other than just pain and stiffness in the neck such as: nausea, dizziness, headaches, ringing in the ears, concussion, etc.
Whiplash Associated Disorder (WAD), describes a more serious and chronic condition which can include symptoms other than just pain and stiffness in the neck such as: nausea, dizziness, headaches, ringing in the ears, concussion, etc.
In automobile accidents, the most common form of impact for whiplash is a rear end type of impact. There are many factors contributing to the injury including: speed of impact, type of seat, type of vehicle, did the occupant brace for impact ? was the occupant looking straight ahead or turned ? etc.
Whiplash can be quantified on X-ray as an "S-Shaped curve":
 It has been well documented that soft tissue structures are injured and which are responsible for localized pain and stiffness. Pain and tingling down the arm(s) can be a sign of a more serious condition such as a cervical disc herniation or a brachial plexus lesion or compression.
It has been well documented that soft tissue structures are injured and which are responsible for localized pain and stiffness. Pain and tingling down the arm(s) can be a sign of a more serious condition such as a cervical disc herniation or a brachial plexus lesion or compression.
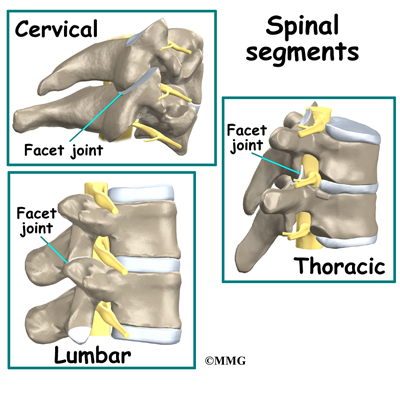
This recent study suggests what Chiropractors have always known, that there is injury to cervical zygapophysial joints OR facet joints following whiplash. Facet joints are located at each level of our vertebrae and are the joints responsible for the "popping or crackling sounds" that we hear from our spines. Facet joints are also the joints that are "adjusted" when Chiropractors manipulate the spine. Perhaps that is why so many patients have found relief with Chiropractic following an automobile accident causing whiplash.
Diagram showing Facet joints:
 Have you been injured in an automobile accident and are suffering from whiplash, headaches or an injury to a spinal disc and nerve ? Call us at (650) 347-2225 to get a correct diagnosis and appropriate treatment. We offer treatment for soft tissue injuries, injuries to the facet joints and cervical disc's. Dr. Hindocha is a Chiropractor in San Mateo who has had over 10 years of experience managing these difficult cases. Moreover, Dr. Hindocha shares his office space with a Physical Medicine & Rehabilitation and Orthopedic specialist should you require advanced care. We offer: Chiropractic care, non-surgical spinal decompression therapy, PT modalities and procedures, therapeutic exercises such as cervical and lumbar core stabilization programs and traction procedures. We will work with your lawyer or can recommend an attorney qualified for your case. Dr. Hindocha's paperwork and medical reports can help support your case to avoid costly litigation.
Have you been injured in an automobile accident and are suffering from whiplash, headaches or an injury to a spinal disc and nerve ? Call us at (650) 347-2225 to get a correct diagnosis and appropriate treatment. We offer treatment for soft tissue injuries, injuries to the facet joints and cervical disc's. Dr. Hindocha is a Chiropractor in San Mateo who has had over 10 years of experience managing these difficult cases. Moreover, Dr. Hindocha shares his office space with a Physical Medicine & Rehabilitation and Orthopedic specialist should you require advanced care. We offer: Chiropractic care, non-surgical spinal decompression therapy, PT modalities and procedures, therapeutic exercises such as cervical and lumbar core stabilization programs and traction procedures. We will work with your lawyer or can recommend an attorney qualified for your case. Dr. Hindocha's paperwork and medical reports can help support your case to avoid costly litigation.
What is Whiplash ?
Whiplash is an injury to the neck and upper back that can occur following an auto accident. Whiplash can also occur in other circumstances where the neck is forced backwards and then forwards such as a fall or during a sporting event. In automobile accidents, whiplash occurs as a result of sudden "acceleration - deceleration" forced to the spine and soft tissue structures (tendons, ligaments and muscles):

In automobile accidents, the most common form of impact for whiplash is a rear end type of impact. There are many factors contributing to the injury including: speed of impact, type of seat, type of vehicle, did the occupant brace for impact ? was the occupant looking straight ahead or turned ? etc.
Whiplash can be quantified on X-ray as an "S-Shaped curve":

This recent study suggests what Chiropractors have always known, that there is injury to cervical zygapophysial joints OR facet joints following whiplash. Facet joints are located at each level of our vertebrae and are the joints responsible for the "popping or crackling sounds" that we hear from our spines. Facet joints are also the joints that are "adjusted" when Chiropractors manipulate the spine. Perhaps that is why so many patients have found relief with Chiropractic following an automobile accident causing whiplash.
Diagram showing Facet joints:
Assessing the outcomes after Spinal Fusion surgery.
From: Perioperative Morbidity and Mortality After Anterior, Posterior, and Anterior/Posterior Spine Fusion Surgery. Stavros G. Memtsoudis, MD, PhD; Vassilios I. Vougioukas, MD, PhD; Yan Ma, PhD; Licia K. Gaber-Baylis, BA; Federico P. Girardi, MD. Spine. 2011;36(22):1867-1877. © 2011 Lippincott Williams & Wilkins.
The utilization of Spinal fusion techniques have increased dramatically despite the relatively few studies showing the safety of this procedure. There is also a relative lack of studies comparing the relative spinal surgical techniques and the outcomes associated with them.
This study was designed to assess the Morbidity (the rate of incidence) and Mortality (the measure of the number of deaths) and to determine the independent risk factors for in-hospital death. associated with the various surgical approaches to spinal fusion surgery.
The outcomes being measured were: Perioperative (after operation) of Anterior Spinal Fusion (ASF), Posterior Spinal Fusion (PSF) and APSF (Anterior Posterior Spinal Fusion).
Here are some X-rays, post-operative:

Results of the study:
There was an increased incidence of perioperative complications and adjusted risk of in-hospital mortality among hospital admissions undergoing APSF and ASF when compared to PSF procedures.
The highest rates of fatal outcomes and complications were associated with procedures using the anterior thoracic approach.
Risk factors for in-hospital mortality included the following: male gender, advanced age, procedures indicated for metastatic disease and trauma, as well as the presence of several comorbidities and perioperative complications.
Procedures involving the anterior spine were associated with higher morbidity and mortality in our study, despite being performed in younger individuals with lower comorbidity burden.
The highest rate of morbidity and mortality was seen in APSF patients, which can be explained by longer surgical times, more blood loss, and increased surgical complexity.
When studying patient demographics and their association with mortality, we found increased independent risk of a fatal event after spine fusion among men.
We identified an increased incidence of morbidity and risk for mortality in patients with advanced age. Patients over the age of 75 years made up almost one- third of all mortalities, despite representing less than 9% of the spine surgical population in this study.
Pulmonary circulatory disease, congestive heart failure, renal disease, and coagulopathies were associated with the highest increases of risk for perioperative mortality.
Perioperative complications were also associated with increases in the odds of a fatal event. Pulmonary embolism, perioperative shock, ARDS, and cardiac complications were associated with the highest risk of mortality. All of these events had the highest incidence among APSF patients.
It was determined that APSF and ASF carried an increased adjusted risk of in-hospital mortality and greater incidence of in-hospital complications when compared to PSF procedures.
What can we learn from this study ? Like the old saying goes "an ounce of prevention equals a pound of cure". Aside from unforeseen circumstances such as trauma, there are ways we can help prevent our spines from getting to this level of degeneration.
1.) Have a spinal exam and check up.
2.) Don't ignore early signs such as: recurring back pain that may self-resolve or resolve with medications. In my experience, most cases of spinal degeneration and herniated discs have manifested themselves in the past and have not been adequately or properly treated. Chiropractic therapy is a drugless, non-surgical, intervention which can help with many types of back pain.
3.) For those of you who have already reached the advanced stages of spinal arthritis, osteroarthritis, degenerative disc disease, sciatica or have one or multiple herniated discs, VAX-D spinal decompression therapy is an alternative approach to some types of surgery and "endless" epidural injections.
4.) Exercise, lose weight and keep a healthy lifestyle.
Dr. Rommel Hindocha is a Chiropractor in San Mateo California. In addition to Chiropractic therapy, he does perform non-surgical Spinal Decompression therapy at 101 S. San Mateo Drive, Suite 200, San Mateo, CA 94401. You can reach Peninsula Spine & Sports Rehabilitation at (650) 347-2225.
The utilization of Spinal fusion techniques have increased dramatically despite the relatively few studies showing the safety of this procedure. There is also a relative lack of studies comparing the relative spinal surgical techniques and the outcomes associated with them.
This study was designed to assess the Morbidity (the rate of incidence) and Mortality (the measure of the number of deaths) and to determine the independent risk factors for in-hospital death. associated with the various surgical approaches to spinal fusion surgery.
The outcomes being measured were: Perioperative (after operation) of Anterior Spinal Fusion (ASF), Posterior Spinal Fusion (PSF) and APSF (Anterior Posterior Spinal Fusion).
Here are some X-rays, post-operative:
Results of the study:
There was an increased incidence of perioperative complications and adjusted risk of in-hospital mortality among hospital admissions undergoing APSF and ASF when compared to PSF procedures.
The highest rates of fatal outcomes and complications were associated with procedures using the anterior thoracic approach.
Risk factors for in-hospital mortality included the following: male gender, advanced age, procedures indicated for metastatic disease and trauma, as well as the presence of several comorbidities and perioperative complications.
Procedures involving the anterior spine were associated with higher morbidity and mortality in our study, despite being performed in younger individuals with lower comorbidity burden.
The highest rate of morbidity and mortality was seen in APSF patients, which can be explained by longer surgical times, more blood loss, and increased surgical complexity.
When studying patient demographics and their association with mortality, we found increased independent risk of a fatal event after spine fusion among men.
We identified an increased incidence of morbidity and risk for mortality in patients with advanced age. Patients over the age of 75 years made up almost one- third of all mortalities, despite representing less than 9% of the spine surgical population in this study.
Pulmonary circulatory disease, congestive heart failure, renal disease, and coagulopathies were associated with the highest increases of risk for perioperative mortality.
Perioperative complications were also associated with increases in the odds of a fatal event. Pulmonary embolism, perioperative shock, ARDS, and cardiac complications were associated with the highest risk of mortality. All of these events had the highest incidence among APSF patients.
It was determined that APSF and ASF carried an increased adjusted risk of in-hospital mortality and greater incidence of in-hospital complications when compared to PSF procedures.
What can we learn from this study ? Like the old saying goes "an ounce of prevention equals a pound of cure". Aside from unforeseen circumstances such as trauma, there are ways we can help prevent our spines from getting to this level of degeneration.
1.) Have a spinal exam and check up.
2.) Don't ignore early signs such as: recurring back pain that may self-resolve or resolve with medications. In my experience, most cases of spinal degeneration and herniated discs have manifested themselves in the past and have not been adequately or properly treated. Chiropractic therapy is a drugless, non-surgical, intervention which can help with many types of back pain.
3.) For those of you who have already reached the advanced stages of spinal arthritis, osteroarthritis, degenerative disc disease, sciatica or have one or multiple herniated discs, VAX-D spinal decompression therapy is an alternative approach to some types of surgery and "endless" epidural injections.
4.) Exercise, lose weight and keep a healthy lifestyle.
Dr. Rommel Hindocha is a Chiropractor in San Mateo California. In addition to Chiropractic therapy, he does perform non-surgical Spinal Decompression therapy at 101 S. San Mateo Drive, Suite 200, San Mateo, CA 94401. You can reach Peninsula Spine & Sports Rehabilitation at (650) 347-2225.
Subscribe to:
Posts (Atom)